The straight leg raise test is a crucial diagnostic tool for assessing lower back and nerve root issues. This in-depth look at the test covers everything from its purpose and variations to the procedure, positive and negative findings, and differential diagnoses. Understanding this test is essential for healthcare professionals and anyone interested in musculoskeletal health.
We’ll delve into the anatomy and physiology behind the test, exploring the relevant structures like the lumbar spine, sciatic nerve, and related muscles. We’ll also discuss the clinical significance of the straight leg raise test in diagnosing and managing lower back pain. This comprehensive guide aims to provide a clear understanding of this important diagnostic technique.
Introduction to the Straight Leg Raise Test
The straight leg raise test, often abbreviated as SLR, is a fundamental neurological examination technique used to assess potential lower back and nerve root issues. It’s a simple maneuver that can elicit pain or other symptoms that indicate the presence of irritation or compression in the lower spine and associated nerves. This test helps clinicians narrow down the potential causes of back pain and other lower extremity symptoms.This test is valuable in evaluating conditions such as herniated discs, spinal stenosis, sciatica, and piriformis syndrome.
The test’s reliability lies in its ability to reproduce symptoms and pinpoint the location of the potential problem within the lower back or sciatic nerve pathway. The specific variations of the test play a crucial role in refining the diagnostic process and targeting the affected area.
Variations of the Straight Leg Raise Test
Different variations of the straight leg raise test provide clinicians with a range of perspectives on the patient’s condition. These variations involve adjusting the patient’s position and the procedure itself.
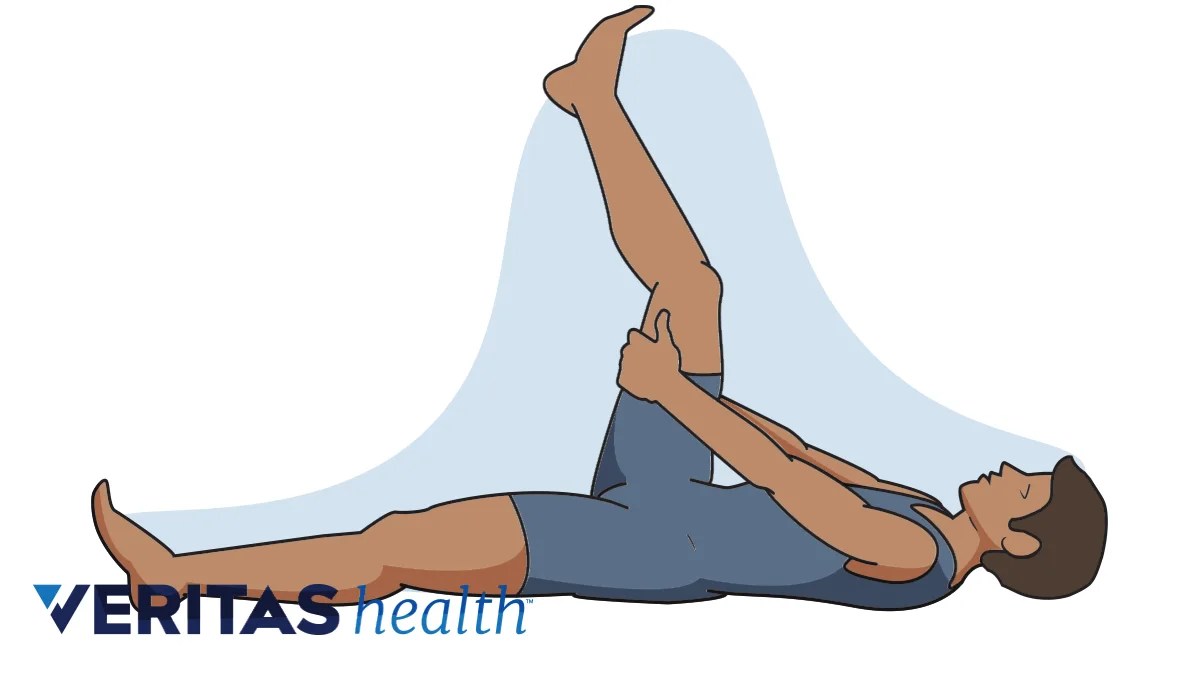
- Supine Straight Leg Raise: This is the most common variation. The patient lies supine (on their back) with one leg extended straight and the other leg flexed at the knee. The examiner then slowly raises the extended leg, keeping it straight, until the patient experiences pain. The angle at which pain begins is crucial in the diagnosis.
- Seated Straight Leg Raise: In this variation, the patient sits on the examination table with one leg extended. The examiner then raises the extended leg, keeping it straight, until the patient experiences pain or discomfort. This variation is particularly useful in assessing the lumbar spine in patients with limited mobility or those who find the supine position uncomfortable.
- Modified Straight Leg Raise (with Dorsiflexion): In this variation, after raising the straight leg, the examiner passively dorsiflexes (pulls up) the foot of the raised leg. This maneuver can increase the pressure on the nerve roots and elicit symptoms that might not be apparent in the standard straight leg raise. This is often used to differentiate between radicular pain (nerve-related) and other types of pain.
Comparison of Straight Leg Raise Variations
The table below summarizes the key differences between the supine, seated, and modified straight leg raise tests.
| Variation | Patient Positioning | Procedure | Expected Findings |
|---|---|---|---|
| Supine Straight Leg Raise | Patient lies supine, one leg extended, other flexed | Examiner raises the extended leg slowly, keeping it straight, until pain is reported. | Pain in the lower back, buttock, or leg. The angle of elevation at which pain occurs is significant. |
| Seated Straight Leg Raise | Patient sits on the table, one leg extended | Examiner raises the extended leg slowly, keeping it straight, until pain is reported. | Pain in the lower back, buttock, or leg. Pain reproduction and the degree of elevation correlate with nerve root impingement. |
| Modified Straight Leg Raise (with Dorsiflexion) | Patient lies supine, one leg extended, other flexed | Examiner raises the extended leg and passively dorsiflexes the foot. | Increased pain or reproduction of symptoms compared to the standard SLR. This strongly suggests nerve root irritation. |
Anatomy and Physiology Related to the Test
The straight leg raise test is a valuable clinical maneuver used to assess potential spinal and nerve-related issues. Understanding the underlying anatomy and physiology is crucial for interpreting the results accurately. This section delves into the relevant structures and mechanisms involved in the test, focusing on the lumbar spine, sciatic nerve, and related muscles.The test elicits pain or discomfort by stretching specific structures, allowing clinicians to identify potential sources of the symptoms.
Proper understanding of the physiological responses to the test is essential for accurate diagnosis and subsequent treatment planning.
Relevant Anatomy of the Lumbar Spine
The lumbar spine comprises five vertebrae, intervertebral discs, ligaments, and muscles. These structures work together to provide stability, flexibility, and support to the spine. The lumbar spine’s stability is crucial for the straight leg raise test as any restrictions or abnormalities can influence the test results. Understanding the specific attachments of muscles and ligaments, and the relationships between vertebrae, is vital in evaluating the results.
Anatomy of the Sciatic Nerve
The sciatic nerve is the largest nerve in the body, originating from the lumbar and sacral plexuses. It branches into numerous smaller nerves, supplying sensation and motor function to the lower limbs. The sciatic nerve’s path through the buttock and posterior thigh is important to consider, as pressure or irritation along this pathway can cause pain or altered sensation, potentially indicated by the straight leg raise test.
Muscle Involvement in the Straight Leg Raise Test
Several muscles contribute to the movement and stability of the lumbar spine during the straight leg raise. Understanding the roles of these muscles is important in interpreting the test results, as their involvement is significant in maintaining spinal alignment and in any potential muscle imbalances that might affect the test. These muscles include the psoas major, iliacus, quadratus lumborum, and hamstrings.
The hamstrings are especially relevant, as their stretch during the test can provoke pain if there’s nerve irritation or inflammation.
Physiological Mechanisms of Pain/Discomfort
Pain during the straight leg raise test can be attributed to several factors. Mechanical compression of nerve roots, inflammation of the sciatic nerve, or tension on ligaments and muscles are potential sources of discomfort. Additionally, muscle spasms and joint restrictions in the lumbar spine can contribute to the observed pain. The test’s effect on the lumbar spine, sciatic nerve, and related muscles is significant.
Neurological Pathways in Response to the Test
The response to the straight leg raise test involves complex neurological pathways. Stimulation of specific sensory receptors in the lower back and legs triggers nerve impulses that travel along afferent pathways to the spinal cord. These impulses are processed in the central nervous system, and a motor response, if any, is initiated. This intricate process allows clinicians to assess the integrity of the nervous system.
Key Anatomical Structures and Their Relationship to the Test
| Anatomical Structure | Relationship to the Test |
|---|---|
| Lumbar Spine (vertebrae, discs, ligaments) | Provides support and stability; movement restrictions can affect test results. |
| Sciatic Nerve | Stretching or irritation of the nerve can cause pain or altered sensation. |
| Psoas Major/Iliacus | Crucial for hip flexion; tension can affect test results. |
| Hamstring Muscles | Stretch during the test; tension or irritation can cause pain. |
| Nerve Roots | Potential compression of nerve roots can produce pain or numbness. |
Procedure and Technique for Performing the Straight Leg Raise Test
The straight leg raise test, a valuable tool in assessing lower back and nerve root issues, relies heavily on precise technique for accurate results. Understanding the procedure, patient positioning, and examiner actions is crucial to avoid misinterpretations and ensure reliable diagnostic information.
Patient Positioning
Proper patient positioning is fundamental for a successful straight leg raise test. The patient should lie supine (on their back) with their knees extended. This ensures that the hamstrings are relaxed and the movement originates from the lumbar spine and sciatic nerve. The hips should be relaxed, and the shoulders and upper back should be flat against the examination table to maintain a neutral spine alignment.
Ever wondered about the straight leg raise test? It’s a common diagnostic tool for lower back pain, and while it’s not directly related to, say, different types of cosmetic dental procedures , understanding your body’s mechanics is key. This simple test helps pinpoint nerve root irritation or other spinal issues. So, next time you’re experiencing discomfort, remember this useful diagnostic tool.
A pillow under the knees may be helpful for patient comfort and to reduce tension in the lower back, if necessary. Ensure the patient feels comfortable and secure in this position. This position eliminates extraneous movement and allows for the evaluation of the lower back and sciatic nerve response.
The straight leg raise test is a common neurological assessment, but did you know that certain conditions, like some types of intellectual disability in children and adults, types of intellectual disability in children and adults , can sometimes impact the results? This is because underlying neurological issues can affect muscle function and reflexes, thus potentially altering the test’s outcome.
The test remains a valuable tool for assessing nerve root irritation, but clinicians should consider the broader context when interpreting the results.
Examiner Technique
The examiner’s technique plays a vital role in the accuracy of the test results. The examiner should ensure a steady and controlled approach to the patient’s leg. The leg being tested should be raised slowly and smoothly, keeping the knee straight throughout the entire movement. The examiner’s hands should be positioned firmly but gently on the patient’s thigh, avoiding any undue pressure or discomfort.
Ever wondered about the straight leg raise test? It’s a simple but surprisingly insightful way to assess lower back and hip issues. Knowing how to interpret the results can be really helpful. If you’re curious about skin concerns, especially if you have skin of color, seeking advice from a qualified dermatologist is key. For example, ask an expert dermatologist for skin of color for tailored advice on skin health and treatment options.
Ultimately, understanding the straight leg raise test can provide valuable clues about your overall physical well-being.
Maintaining consistent pressure throughout the procedure is important. The examiner should observe the patient’s reaction closely for any signs of pain, discomfort, or neurological symptoms. The examiner must maintain a neutral posture to avoid introducing any bias or influence on the test results. Consistency in technique is paramount.
Procedure Steps
This structured approach ensures a standardized procedure for all patients.
- Preparation: Ensure the patient is comfortable and positioned supine on the examination table. Inform the patient about the procedure and obtain their consent. Make sure the room is adequately lit and the patient feels relaxed.
- Examiner Positioning: Position yourself strategically to maintain a comfortable reach to the patient’s leg without straining.
- Leg Elevation: The examiner should slowly and steadily raise the patient’s leg, keeping the knee straight. Avoid jerking or forceful movements.
- Observation: Pay close attention to the patient’s facial expression, posture, and any verbal cues indicating pain or discomfort. Observe for any resistance or tightness in the lower back.
- Recording: Note the degree of leg elevation at which the patient experiences pain or discomfort. Document the specific location and type of pain reported by the patient.
- Repeat: Repeat the procedure on the other leg, following the same technique and recording observations. This ensures symmetry and comparative analysis.
Common Errors and Implications
Several errors can compromise the accuracy of the straight leg raise test.
- Jerking or Forceful Movements: Jerky movements during leg elevation can lead to inaccurate readings as the patient may react to the sudden change in position. This can cause discomfort or masking of actual pain points.
- Insufficient Support: Lack of proper support for the patient’s back can lead to compensatory movements from the patient, affecting the reliability of the results.
- Pressure on the Knee: Excessive pressure on the patient’s knee during leg elevation can cause discomfort and alter the response. The examiner must maintain a gentle touch.
- Failure to Maintain a Straight Knee: Allowing the knee to bend during the leg raise introduces an extraneous variable that masks the true pain response from the lower back or sciatic nerve. The examiner must ensure the knee remains straight throughout the procedure.
Table of Procedure Steps
| Step | Examiner Action | Patient Action |
|---|---|---|
| 1 | Position patient supine, ensure comfort | Lie still and relaxed on back |
| 2 | Position self for easy access to patient’s leg | Remain still |
| 3 | Slowly raise patient’s leg, keeping knee straight | Remain still and report any pain or discomfort |
| 4 | Observe patient’s response for pain or discomfort | Report any pain or discomfort |
| 5 | Record the degree of leg elevation at which pain occurs | Report any pain or discomfort |
| 6 | Repeat steps 3-5 for the opposite leg | Remain still and report any pain or discomfort |
Positive and Negative Findings of the Straight Leg Raise Test
The straight leg raise test, a valuable diagnostic tool in assessing lower back and nerve root pain, provides crucial insights into potential underlying pathologies. Understanding the nuances of positive and negative findings allows healthcare professionals to effectively interpret the results and guide appropriate treatment strategies. This section delves into the specifics of these findings, emphasizing the significance of pain location and intensity during different degrees of leg elevation.
Positive Findings
The straight leg raise test is considered positive when pain is elicited. The pain experienced during the test can vary in location and intensity, offering valuable clues about the affected area.
- Pain in the low back: Pain localized to the low back, particularly during the early stages of leg elevation, might suggest a problem with the lumbar spine itself, such as a herniated disc, spinal stenosis, or facet joint dysfunction. The specific level of the back where the pain is felt can help pinpoint the area of concern. For example, pain in the lower lumbar region (L4-L5) might indicate issues with these specific vertebrae.
- Pain radiating down the leg: Pain that travels down the leg, often following the distribution of a specific nerve root, is a strong indicator of nerve root irritation or compression. This is a hallmark of sciatica, a condition often caused by a herniated disc pressing on a nerve root. The pattern of pain (e.g., burning, sharp, tingling) can provide additional information about the nature of the issue.
- Pain worsening with further elevation: If the pain intensifies as the leg is raised further, it suggests that the affected nerve root is being stretched or compressed more significantly. This can be a critical factor in differentiating between different causes of pain. For instance, a gradual increase in pain during the test may point towards a gradual pressure buildup on the nerve root.
- Pain at a specific point in the leg: The exact location of pain down the leg can help pinpoint the specific nerve root that is being affected. For example, pain in the anterior thigh suggests involvement of the femoral nerve, whereas pain in the lateral aspect of the leg might indicate involvement of the superior gluteal nerve.
Negative Findings
A negative straight leg raise test, where no pain is elicited, doesn’t necessarily rule out pathology entirely. However, it can suggest the absence of certain types of nerve root irritation or compression.
- Absence of pain: The absence of pain during the entire range of motion can suggest that the nerve roots are not significantly affected. This doesn’t mean there aren’t other potential issues, as other musculoskeletal structures may be involved.
- Pain in the hip or buttock: Pain localized to the hip or buttock during the test might indicate a musculoskeletal problem in these areas rather than nerve root irritation. This could include issues with the hip joint, muscles, or tendons.
Significance of Pain During Different Degrees of Leg Elevation
The degree of leg elevation at which pain occurs is important for interpretation.
- Early elevation pain: Pain that appears early in the range of motion (less than 30 degrees) might suggest a problem with the lumbar spine itself or in the area around the sciatic nerve. A patient experiencing pain at this point is likely not suffering from nerve compression.
- Mid-range elevation pain: Pain that arises in the mid-range of elevation (30-70 degrees) often indicates a potential herniated disc or other spinal conditions pressing on a nerve root. This is a more specific indicator for possible nerve root irritation.
- High elevation pain: Pain that occurs only at higher elevations (greater than 70 degrees) might suggest other causes of hip pain, such as problems with the hip joint itself.
Interpreting Results
The interpretation of the straight leg raise test results should always be done in conjunction with other clinical findings, including the patient’s history and physical examination. The specific location and nature of the pain are crucial for a proper diagnosis.
| Finding | Description | Possible Implications |
|---|---|---|
| Positive (Pain in low back) | Pain localized to the low back during early leg elevation | Lumbar spine pathology (e.g., herniated disc, facet joint dysfunction) |
| Positive (Radiating pain down the leg) | Pain radiating down the leg, following nerve root distribution | Nerve root irritation or compression (e.g., sciatica) |
| Negative (No pain) | Absence of pain throughout the range of motion | Absence of significant nerve root irritation or compression; other pathology possible |
| Positive (Pain in hip/buttock) | Pain localized to the hip or buttock | Musculoskeletal problem in the hip region (e.g., hip joint issues, bursitis) |
Differential Diagnoses and Related Conditions
The straight leg raise test (SLRT) is a valuable diagnostic tool, but it’s crucial to understand that a positive result doesn’t definitively diagnose lumbar radiculopathy. Several other conditions can produce similar symptoms, making accurate differential diagnosis essential. Interpreting the SLRT requires careful consideration of the patient’s complete history, physical examination findings, and potentially, further imaging studies.Understanding the potential for false positives allows for more nuanced and accurate interpretations of the test results.
A thorough understanding of the conditions that can mimic lumbar radiculopathy is critical for avoiding misdiagnosis and ensuring appropriate treatment.
Conditions Mimicking Lumbar Radiculopathy
Several conditions can produce symptoms similar to those of lumbar radiculopathy, potentially leading to a misdiagnosis if the SLRT is not interpreted in the context of the entire clinical picture. These conditions can affect the lumbar spine, pelvis, or even the hip, leading to pain radiating down the leg.
- Hip Pathology: Conditions such as hip osteoarthritis, bursitis, or labral tears can cause pain that mimics radicular pain. The pain may radiate down the leg, but the mechanism is different from nerve impingement in the lumbar spine. The SLRT may be positive, but the absence of other neurological deficits (like weakness, numbness, or reflex changes) and a focused history of hip pain might suggest hip pathology as the primary source.
- Piriformis Syndrome: The piriformis muscle, located deep in the buttock region, can compress the sciatic nerve. This compression can cause pain radiating down the leg, similar to lumbar radiculopathy. The pain is often unilateral, and the SLRT may be positive. However, piriformis syndrome is typically associated with pain that worsens with prolonged sitting or with activities that involve the buttock muscles.
- Spinal Stenosis: Narrowing of the spinal canal can compress the nerves, causing pain and radiating symptoms. While the pain might be similar to lumbar radiculopathy, spinal stenosis typically presents with symptoms that worsen with extension of the spine (bending backward) rather than flexion (bending forward). This difference in the pattern of pain can be crucial for differentiating it from lumbar radiculopathy, where pain often worsens with flexion.
- Sacroiliac Joint Dysfunction: Pain originating from the sacroiliac joint can radiate down the leg, mimicking radicular pain. The SLRT may be positive, but the pain is often localized to the buttock or lower back region. The absence of neurological deficits and tenderness over the sacroiliac joint may be important clues in diagnosing this condition.
Role of the Straight Leg Raise Test in Differential Diagnosis
The SLRT’s value lies in its ability to suggest the presence of nerve root irritation. It helps narrow down the possibilities and guide further investigation. However, it’s not a definitive diagnostic test. It should be used in conjunction with a thorough patient history, a comprehensive neurological examination, and potentially, imaging studies (such as MRI or X-rays) to reach an accurate diagnosis.
- Differentiating between Conditions: Comparing the findings of the SLRT with other physical exam findings and patient history can help differentiate between lumbar radiculopathy and other conditions. For example, if the patient reports pain that is worse with prolonged sitting or activities involving the buttock muscles, piriformis syndrome is more likely than lumbar radiculopathy.
- Example Scenarios: A patient with a positive SLRT, but also reports pain that is significantly worse with standing and walking, may indicate spinal stenosis. Conversely, a patient with a positive SLRT, but no neurological deficits and tenderness over the sacroiliac joint, may suggest sacroiliac joint dysfunction.
Differential Diagnoses Table, Straight leg raise test
| Differential Diagnosis | Characteristics | Relationship to Straight Leg Raise Test |
|---|---|---|
| Lumbar Radiculopathy | Pain radiating down the leg, associated with neurological deficits (weakness, numbness, decreased reflexes). | Often positive, but not always. |
| Hip Pathology | Pain localized to the hip, may radiate down the leg. | May be positive, but often without neurological deficits. |
| Piriformis Syndrome | Pain radiating down the leg, often worse with prolonged sitting or buttock activities. | May be positive, but often with tenderness over the piriformis muscle. |
| Spinal Stenosis | Pain radiating down the leg, worse with extension of the spine. | May be positive, but often with symptoms worsened by extension. |
| Sacroiliac Joint Dysfunction | Pain localized to the buttock or lower back, may radiate down the leg. | May be positive, but often without neurological deficits. |
Clinical Significance and Applications: Straight Leg Raise Test
The straight leg raise test (SLRT) is a valuable clinical tool for assessing lower back pain and potential nerve root impingement. Its simplicity and relative ease of performance make it a cornerstone in the initial evaluation of patients presenting with such complaints. Understanding the test’s clinical relevance, its role in guiding further investigations, and how its findings impact treatment strategies is crucial for effective patient management.The straight leg raise test is a physical examination technique used to detect nerve root irritation or compression in the lumbar spine.
It helps clinicians narrow down the potential causes of lower back pain and guide subsequent diagnostic procedures. The test’s reliability, combined with its sensitivity to specific conditions, allows for more targeted interventions and improved patient outcomes.
Clinical Relevance in Lower Back Pain
The straight leg raise test’s sensitivity in identifying nerve root irritation makes it a critical component in evaluating lower back pain. A positive result, characterized by pain radiating down the leg, suggests possible nerve root involvement. This information is vital for differentiating between various causes of lower back pain, ranging from simple muscle strains to more serious conditions like herniated discs or spinal stenosis.
The test helps clinicians focus their diagnostic efforts on conditions that are likely to cause nerve root irritation, thus reducing the likelihood of misdiagnosis.
Role in Guiding Further Investigations
A positive SLRT often prompts further investigations to confirm the suspected diagnosis and determine the appropriate treatment plan. The test results provide crucial information for deciding whether imaging studies, such as X-rays, CT scans, or MRIs, are necessary. The test can also guide the need for neurological assessments, like electromyography (EMG) or nerve conduction studies, to evaluate the extent of nerve damage or compression.
This targeted approach helps in achieving a precise diagnosis and avoiding unnecessary and potentially costly procedures. For example, a negative SLRT in a patient with persistent lower back pain might suggest a non-radicular cause, such as a facet joint problem, leading to a different set of investigations.
Influence on Treatment Strategies
The findings of the straight leg raise test directly influence the chosen treatment strategies. A positive test result, indicative of nerve root irritation, may necessitate conservative treatments like physical therapy, pain management, or medication. Surgical intervention might be considered if conservative measures fail to alleviate the symptoms. The degree of pain and the specific location of the radiating pain, as elicited during the test, can help determine the appropriate treatment approach.
For instance, if the pain is severe and localized to the posterior thigh, it might suggest a more immediate need for intervention compared to pain in the calf.
Importance of Combining with Other Clinical Assessments
The straight leg raise test is most effective when combined with other clinical assessments, such as palpation, range of motion tests, and neurological examinations. These combined assessments provide a more comprehensive picture of the patient’s condition. For instance, the combination of a positive SLRT with a diminished ankle reflex may suggest a more significant nerve root compression than a positive SLRT alone.
This comprehensive approach helps to avoid misdiagnosis and ensures the most appropriate treatment is initiated.
Clinical Scenarios and Diagnostic Value
| Clinical Scenario | Positive SLRT Finding | Diagnostic Value |
|---|---|---|
| Herniated Disc | Pain radiating down the leg, often worse with extension | High suspicion for nerve root impingement; further imaging likely required. |
| Spinal Stenosis | Pain increasing with extension or prolonged standing | Suggests narrowing of the spinal canal; further imaging essential. |
| Spondylolisthesis | Pain radiating down the leg, often worse with flexion | May indicate a slipped vertebra; imaging to evaluate the degree of slippage. |
| Sciatica | Pain radiating along the sciatic nerve | Suggests irritation of the sciatic nerve; further assessment to rule out other conditions. |
| Muscle Strain | No radiating pain, localized pain | Suggests a muscular issue; other physical examination techniques would be needed to rule out other causes. |
Ending Remarks

In conclusion, the straight leg raise test, while seemingly simple, offers valuable insights into lower back and nerve root conditions. Understanding its procedure, potential findings, and differential diagnoses empowers healthcare professionals to make informed decisions. This guide highlights the crucial role of the test in diagnosing and managing lower back pain, emphasizing the importance of accurate interpretation and combining it with other clinical assessments.
By mastering this test, you can contribute to a more effective and comprehensive approach to patient care.









