
The landscape of public healthcare in the United States is poised for a significant transformation as states prepare for the implementation of the 2025 federal reconciliation law. This legislation introduces a mandatory work requirement for adults within the Affordable Care Act (ACA) Medicaid expansion group, as well as those enrolled in partial expansion waiver programs. For California, which manages the nation’s largest Medicaid program, known as Medi-Cal, the stakes are uniquely high. Starting January 1, 2027, the state must condition eligibility on meeting specific work or community engagement criteria, a move that necessitates a massive overhaul of administrative systems, enrollee communication strategies, and fiscal planning.
As California officials begin the multi-year process of transitioning to this new regulatory framework, they do so against a backdrop of tightening fiscal constraints. The state is currently grappling with slowing revenue growth and the expiration of pandemic-era federal subsidies, creating a precarious environment for a program that serves nearly 15 million residents. The intersection of federal mandates and state-level budget deficits is forcing California to make difficult choices regarding coverage, benefits, and administrative investments.
The Federal Mandate and the 2025 Reconciliation Law
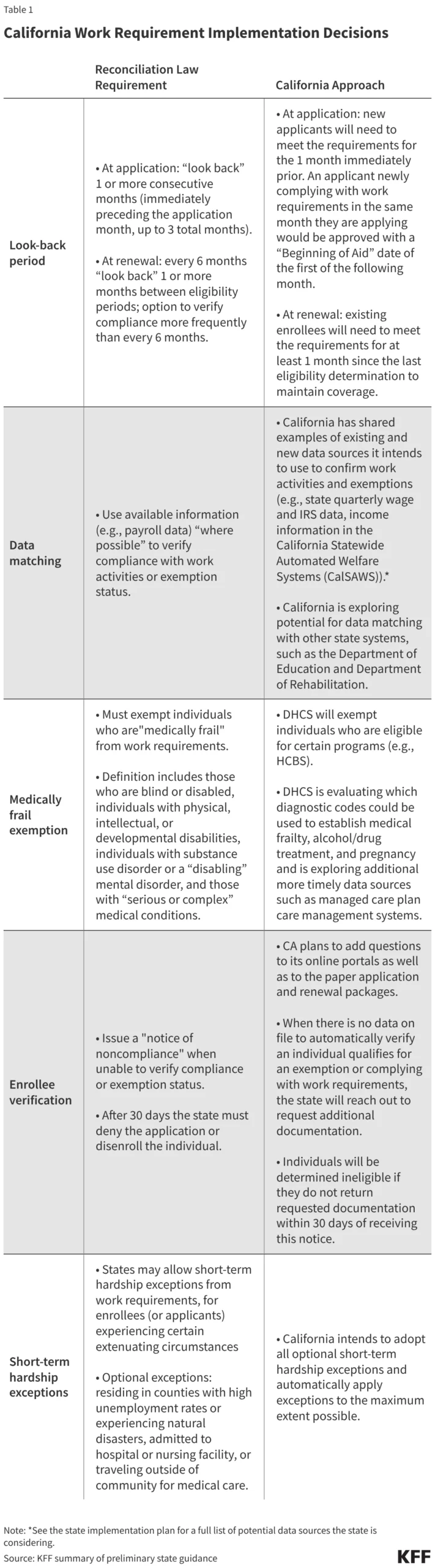
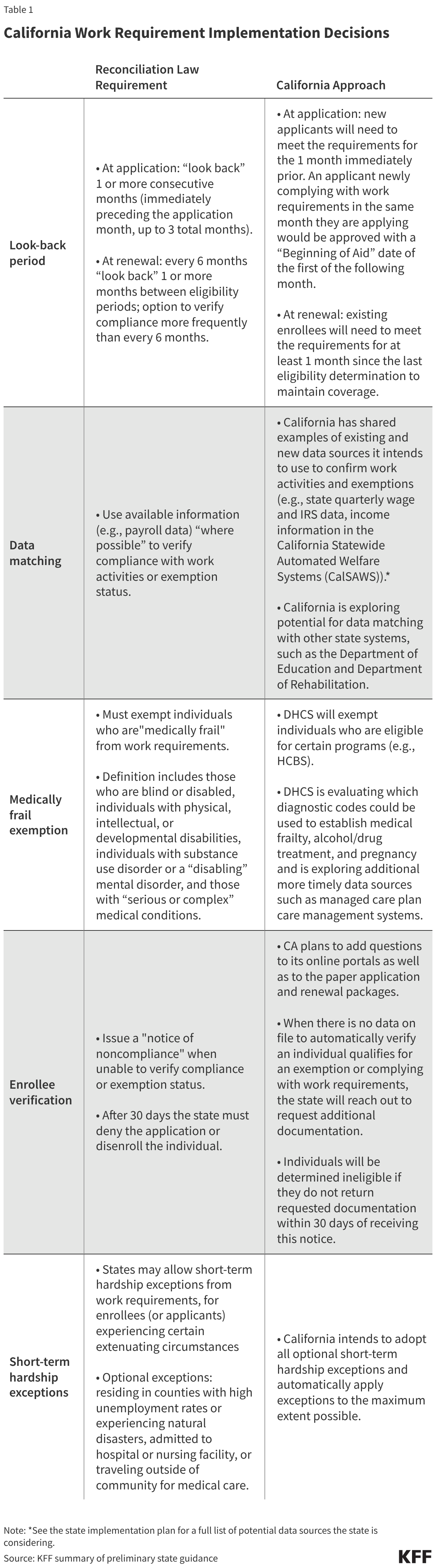
The 2025 reconciliation law represents one of the most substantial shifts in Medicaid policy since the passage of the ACA. By requiring states to implement work requirements for the expansion population, the federal government is introducing a level of administrative complexity that has historically led to significant fluctuations in enrollment. Under the new law, adults subject to the requirement must demonstrate at least 80 hours per month of employment, education, or qualifying community service.
For California, this mandate applies to the roughly five million individuals who gained coverage through the ACA expansion. While the law includes certain exemptions—such as for those who are "medically frail," caregivers, or students—the burden of proof falls on the state and the enrollees to verify compliance. This process requires a sophisticated data-matching infrastructure that can interface with labor departments, educational institutions, and social service agencies in real-time.
California’s Fiscal Outlook: From Surplus to Structural Deficit
The timing of the federal mandate coincides with a period of significant economic adjustment for the Golden State. After several years of record-breaking revenue and expenditure growth fueled by post-pandemic recovery and federal stimulus, California’s fiscal climate has cooled. Governor Gavin Newsom’s administration recently projected a $3 billion structural deficit for fiscal year (FY) 2027, a figure that is expected to balloon to $22 billion by FY 2028 if current spending and revenue trends continue.
The governor’s proposed budget attributes much of this fiscal pressure to the 2025 reconciliation law. The administration estimates that the law will result in a $1.4 billion hit to the General Fund in FY 2027 alone, with $1.1 billion of that impact concentrated within the Medicaid program. These costs stem from a combination of reduced federal matching funds and the increased administrative overhead required to implement the new eligibility rules.
In response to these pressures, the state has already begun implementing cost-containment measures. In FY 2026, California moved to slow Medicaid spending by restoring the asset test for seniors and persons with disabilities—a requirement that had previously been eliminated to simplify eligibility. Additionally, the state ended Medicaid coverage for GLP-1 medications used specifically for obesity treatment and phased out supplemental payments for dental services. These "base spending" adjustments are designed to preserve the core functions of Medi-Cal while bracing for the larger fiscal shocks expected in 2027.
Chronology of Implementation and Key Milestones
The road to January 2027 is marked by several critical administrative and legislative milestones. The state’s Department of Health Care Services (DHCS) has already begun releasing preliminary guidance and implementation plans to provide a roadmap for stakeholders.
- June 2025: California reports 14.8 million total Medi-Cal enrollees, setting the baseline for the expansion population affected by the new law.
- December 2025: The expiration of enhanced ACA Marketplace premium tax credits occurs, prompting the state to allocate local funds to maintain subsidies for low-income residents.
- March 2026: The Medicaid Advisory Committee (MAC) holds pivotal meetings to outline outreach and communication plans, emphasizing the need for multi-lingual and multi-channel notification systems.
- Late 2026: States are required to begin "pre-outreach" to notify individuals of the upcoming requirements at least three months before the first compliance "look-back" period begins.
- January 1, 2027: Official commencement of Medicaid work requirements for the ACA expansion group.
Demographic Profile and the Risk of Disenrollment
A central concern for health policy analysts and advocates is the potential for large-scale disenrollment due to administrative "churn" rather than actual ineligibility. Data from KFF indicates that a majority of the expansion population in California is already meeting the spirit of the work requirement. Approximately 63% of Medicaid adults without dependent children in the state are either working more than 80 hours per month or are enrolled in school.
However, the remaining 37%—representing nearly 1.8 million people—may face significant hurdles. This group includes individuals with chronic health conditions that do not meet the strict federal definition of disability, those with volatile gig-economy schedules, and individuals living in rural areas with limited employment opportunities. California’s own estimates suggest that the introduction of work requirements could result in up to 1.4 million individuals being disenrolled over the implementation period.
The risk is particularly high for those who are eligible for exemptions but fail to navigate the bureaucratic process of claiming them. The "medically frail" exemption, for instance, requires clinical verification that can be difficult to obtain for those with limited access to primary care providers.
Administrative Readiness and Systemic Challenges
The success of California’s implementation hinges on its Information Technology (IT) infrastructure and its ability to perform ex parte renewals—a process where the state verifies eligibility through existing data sources without requiring the enrollee to submit paperwork.
As of late 2025, California’s performance metrics showed a mixed bag of readiness. While nearly 90% of applications were processed within the 30-day window, and 73% of renewals were handled through ex parte processes, a staggering 92% of those who were disenrolled lost coverage for "procedural reasons." Procedural disenrollments occur when an individual may still be eligible but is terminated because they did not return a form or the state had an incorrect mailing address.
State officials acknowledge that the work requirements will exponentially increase the manual administrative workload. To mitigate this, the Governor’s budget includes $4 million for "navigators"—community-based workers tasked with helping enrollees understand the new rules and submit necessary documentation. However, critics argue that $4 million is a modest sum given the scale of the 5-million-person expansion population.
Local Responses and the Rural-Urban Divide
The impact of the 2025 reconciliation law is not being felt uniformly across the state. Rural areas, which often have higher proportions of Medicaid enrollees and fewer administrative resources, are particularly vulnerable. While California received $233 million from the federal Rural Health Transformation Program, these funds are viewed as a temporary "band-aid" rather than a long-term solution for the projected funding gaps.
In a notable shift toward local self-reliance, voters in some California counties have begun taking matters into their own hands. In December 2025, one county approved a ballot measure to increase local sales taxes specifically to backfill Medicaid funding cuts caused by the reconciliation law. Several other counties are reportedly considering similar measures for the 2026 election cycle, suggesting a growing trend of "decentralized" healthcare funding to preserve local safety nets.
Broader Implications and Analysis
The implementation of Medicaid work requirements in California serves as a high-stakes experiment in social policy and fiscal management. Beyond the immediate impact on enrollees, the shift has broader implications for the state’s healthcare ecosystem:
- Provider Stability: Hospitals and community clinics, particularly those in low-income areas, rely heavily on Medi-Cal reimbursements. A sudden drop of 1.4 million enrollees could lead to a surge in uncompensated care, threatening the financial viability of "safety-net" providers.
- Labor Market Effects: While the stated goal of work requirements is to encourage employment, economic research on previous state-level experiments (such as in Arkansas) suggests that these mandates often fail to increase employment while successfully reducing healthcare access.
- State-Funded Programs: In a move that mirrors the federal mandate, Governor Newsom has proposed applying work requirements to the state-funded health program for undocumented immigrants. This suggests a broader policy shift within California toward "personal responsibility" models, even for programs entirely under state control.
As 2027 approaches, California finds itself at a crossroads. The state must balance its historical commitment to broad healthcare access with the rigid mandates of federal law and the realities of a tightening budget. The coming months will be defined by intense administrative preparation, as the state attempts to build a system that can distinguish between those who are truly ineligible and those who are simply lost in the red tape of a massive bureaucratic transition.



{kind=link}