
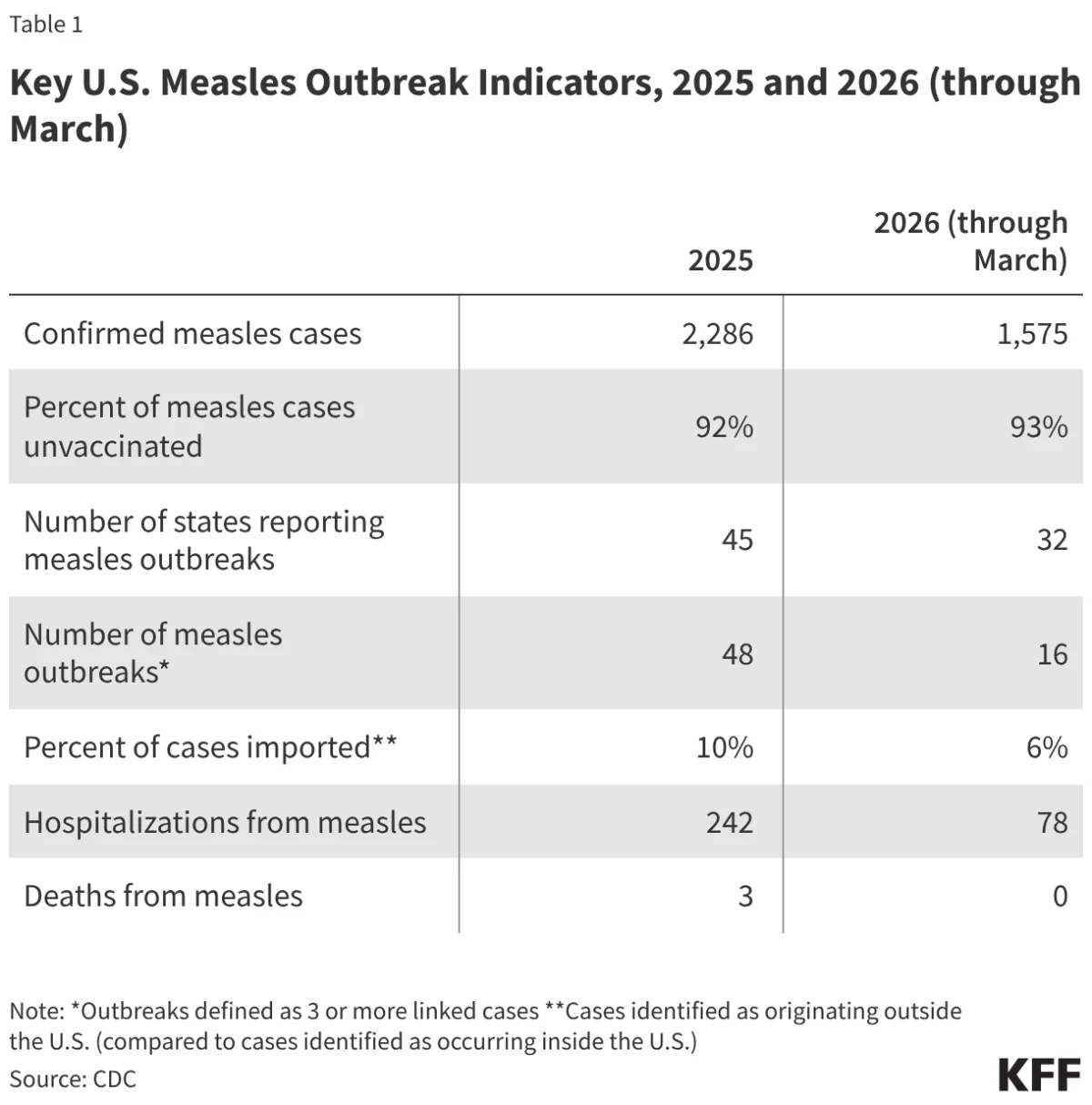
The United States stands at a precarious public health crossroads as the resurgence of measles threatens to dismantle a clinical milestone held for over a quarter of a century. Since the year 2000, measles has been classified as "eliminated" in the U.S., a designation signifying that the virus was no longer endemic and that continuous, year-long domestic transmission had been successfully interrupted. However, a relentless series of outbreaks that began in January 2025 has persisted into the second quarter of 2026, forcing health authorities to confront the possibility that the nation may lose its elimination status. From the start of 2025 through March 2026, state health departments have confirmed more than 3,800 cases of measles, a figure that dwarfs the annual averages of the previous two decades.
This resurgence is not merely a statistical anomaly but the result of a complex interplay between eroding public health infrastructure, shifting political messaging, and a significant decline in pediatric vaccination rates. As the Measles and Rubella Elimination Regional Monitoring and Re-Verification Commission (MRE-RVC) of the Pan American Health Organization (PAHO) prepares for a formal review in late 2026, the data suggests that the U.S. is struggling to contain a pathogen that is among the most contagious known to science.
The Path to Elimination and the Definition of Success
To understand the gravity of the current situation, it is necessary to define what "elimination" means in a modern epidemiological context. Unlike eradication, which refers to the global extinction of a pathogen (as achieved with smallpox), elimination refers to the interruption of endemic transmission in a specific geographic area for 12 months or longer. For a country to maintain this status, any cases that occur must be linked to international "importations" and must not result in a sustained chain of domestic transmission lasting more than a year.
The U.S. first set a goal to eliminate measles in 1966, shortly after the first vaccine became available. While it took decades of refined immunization strategies, the goal was officially reached in 2000. This achievement was re-verified in 2011 by an external panel of experts who found that the combination of high-quality surveillance and a robust two-dose vaccination program—boasting coverage levels near 95%—was sufficient to keep the virus at bay.
For 25 years, the U.S. successfully contained small clusters of cases, usually brought in by travelers. Even during the significant 2018-2019 outbreaks, which saw over 1,200 cases centered in New York, aggressive local intervention and clear federal messaging managed to break the chain of transmission within the 12-month window. The current crisis, however, presents a different trajectory, with transmission chains appearing more durable and harder to trace.
Chronology of the 2025-2026 Resurgence
The current crisis began in early 2025, with an initial cluster of cases identified in West Texas. Unlike previous years where outbreaks were quickly isolated, the 2025 cases spread rapidly across state lines, fueled by communities with significant "immunity gaps." By the end of 2025, the U.S. had recorded 48 distinct outbreaks.
In early 2026, the momentum of the virus showed no signs of slowing. Between January and March 2026 alone, 16 new outbreaks were reported. A critical shift in the epidemiology of these cases has been noted by the Centers for Disease Control and Prevention (CDC): while historically about 40% of U.S. measles cases were imported from other countries, in 2025, only 10% were imported. In the first three months of 2026, that number dropped to 6%. This indicates that the vast majority of cases are now the result of local, domestic transmission, a hallmark of endemicity.
The severity of the current cycle is also reflected in clinical outcomes. Of the confirmed cases in 2025, approximately 13% resulted in hospitalizations. Three deaths were recorded in 2025, the highest number of measles-related fatalities the U.S. has seen in decades. This highlights the reality that measles is not a benign childhood illness; it can lead to pneumonia, encephalitis, and permanent immune system damage, a phenomenon known as "immune amnesia" that leaves children vulnerable to other infections for years after recovery.
The Vaccination Gap and Public Skepticism
The primary defense against measles is the Measles, Mumps, and Rubella (MMR) vaccine, which is 97% effective after two doses. To achieve "herd immunity"—the point at which the virus cannot find enough susceptible hosts to spread—a population must maintain a vaccination rate of at least 95%.
Recent data reveals that the U.S. has fallen dangerously below this threshold. National two-dose MMR coverage for children entering kindergarten in 2024 was estimated at 92.5%, a steady decline from the 94.7% reported in 2011. The national average masks even more dire local statistics; in some states like Idaho, coverage has dropped as low as 78.5%. In 2024, only 10 states reported meeting or exceeding the 95% target.
This decline is inextricably linked to a broader erosion of trust in health authorities. Public health polling in 2025 and 2026 indicates that nearly 20% of adults believe the false claim that the measles vaccine is more dangerous than the disease itself. Misinformation, often amplified on social media, has complicated outreach efforts, making it difficult for health officials to persuade parents in high-risk communities to adhere to immunization schedules.
Infrastructure and Leadership Challenges
The public health response to the 2025-2026 outbreaks has been hampered by significant administrative and financial hurdles. Federal, state, and local health departments have faced budget cuts and staffing shortages, reducing their capacity for the intensive contact tracing required to contain measles. Historically, the federal government provided over 50% of the funding for state and local public health departments; recent reductions have left these agencies under-resourced at a time of peak demand.
Furthermore, a vacuum in federal leadership has led to inconsistent messaging. The CDC was without a Senate-confirmed director for the majority of the period since the outbreaks began. During this interval, Department of Health and Human Services (HHS) Secretary Robert F. Kennedy, Jr. has faced criticism for downplaying the risks of measles and suggesting alternative treatments over vaccination.
While acting CDC Director Jay Bhattacharya issued strong statements in March 2026 reaffirming that vaccination is the most effective way to protect communities, previous comments from other high-ranking officials described the outbreaks as a "cost of doing business" and a matter of "personal freedom." This lack of a unified, authoritative voice has contrasted sharply with the 2019 response, where bipartisan and inter-agency messaging was clear and focused on the urgency of immunization.
Regional and Global Context
The U.S. experience is part of a larger North American trend. In November 2025, PAHO officially declared that Canada had lost its measles elimination status following more than 12 months of uncontrolled transmission. Mexico also reported over 6,200 cases in 2025. Globally, measles activity has surged, with the World Health Organization (WHO) reporting over 276,000 cases in the first half of 2026, with massive outbreaks in Europe, the Eastern Mediterranean, and parts of Africa.
This global surge creates a feedback loop: as the virus circulates more widely abroad, the risk of "importation" into the U.S. increases. When these imported cases land in U.S. communities with low vaccination rates, they spark the domestic chains of transmission that are currently threatening the nation’s 26-year streak of elimination.
Implications of Losing Elimination Status
As the November 2026 PAHO review approaches, the CDC is conducting advanced genomic sequencing to determine if the cases across various states are epidemiologically linked to a single, continuous chain of transmission—specifically the outbreak that began in Texas in January 2025. If the virus has been circulating uninterrupted for over a year, the formal loss of elimination status is likely.
The consequences of such a downgrade would be profound. Economically, the cost of managing endemic measles is significantly higher than the cost of maintaining elimination. Outbreak response requires thousands of hours of public health labor, expensive quarantine measures, and places a strain on hospital systems.
Socially, a return to endemic measles would mean that schools, daycares, and healthcare facilities would face more frequent disruptions. For the most vulnerable—infants too young to be vaccinated and immunocompromised individuals—the risk of severe illness or death would become a permanent fixture of daily life rather than a rare threat.
The loss of elimination status would ultimately serve as a signal that the infrastructure and social contract required to maintain public health are fracturing. Reclaiming that status would require not only a renewed investment in health funding but also a concerted effort to rebuild public trust in the science of immunization. As the 2026 outbreaks continue, the window for intervention is narrowing, placing the U.S. at risk of surrendering one of its greatest public health achievements of the 21st century.


{kind=link}